



Introducing Ion
Introducing Ion
Getting answers
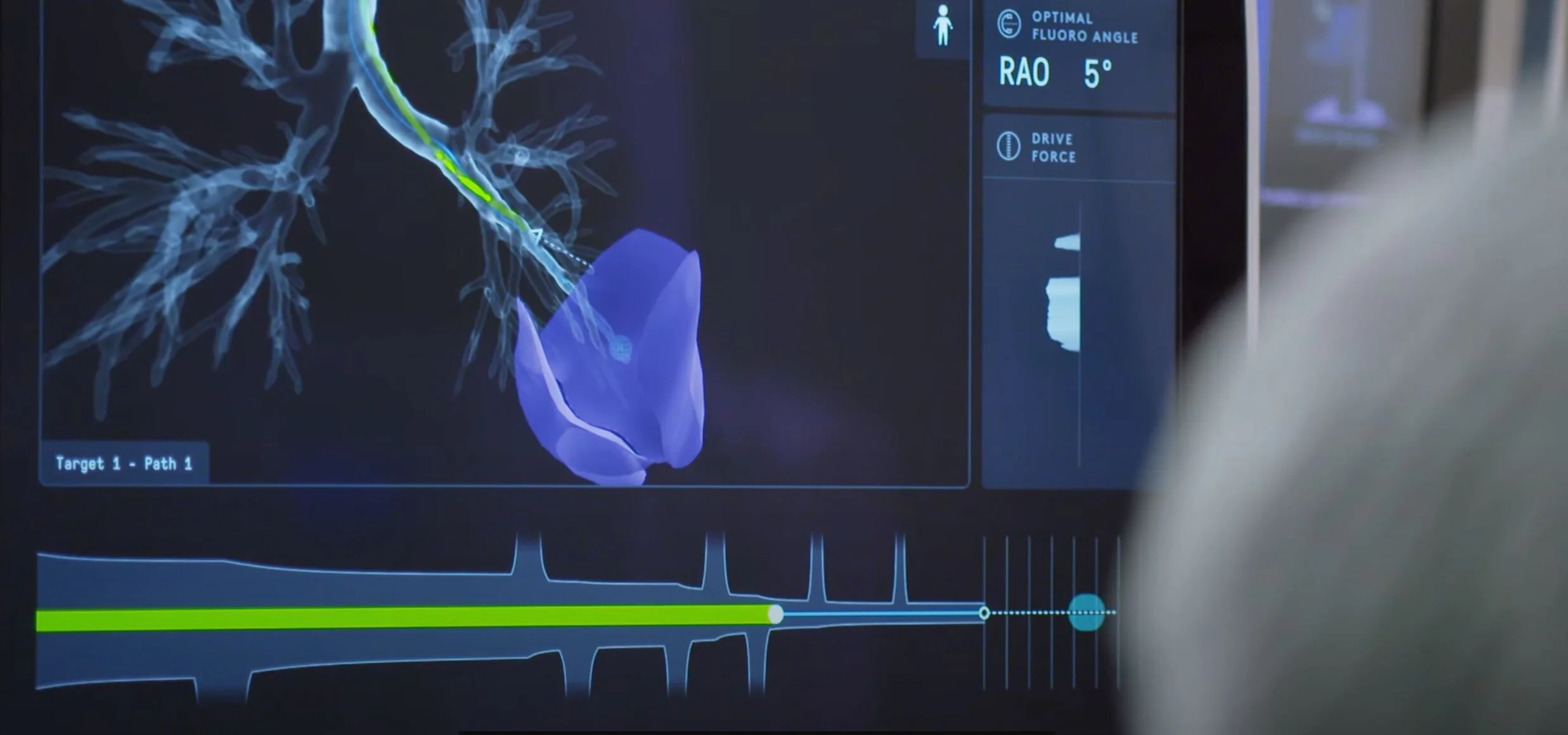
Around the world, lung cancer is on the rise. Today, when a physician finds a small lesion on a patient’s lung, they have few options to perform a biopsy for tissue diagnosis. We recognized that innovation was needed to provide a minimally invasive solution with higher yield than previous approaches. The challenges are great: Early stage cancers are small in size and can be located anywhere in the lung, but are most often located in the outer 1/3—far out of reach of traditional bronchoscopy tools. In many cases, these existing methods require tools that are either too large or too limited to position accurately in the peripheral lung where airways can branch out to sizes less than 2mm in diameter. Also many lesions form outside the airway walls, where they cannot be seen by direct line of sight. Even if a physician can get close, they often must rely on limited external imaging and sensor technology to estimate where the lesion is in relation to the catheter.

Navigating the lung
Navigating the lung
Biopsy workflow
While it is true that the Ion system brings something entirely new to the bronchoscopy suite, we believe its success depends on how well the technology can fit into existing environments and workflows. We took this into account in the design.
Portability and small footprint were key objectives so the system could be nimble enough to be placed in a standard bronchoscopy suite setup without requiring special accommodations. Our technology is designed to easily enter the room when required and leave the room when it is not. We also made sure to preserve the ability for the clinicians to work where they wanted to work—ensuring physical access to each other and to the patient. Using the Ion system does not mean standing off to the side with a piece of equipment.



More Reach
More Reach
Macro and micro
After half a decade of searching for designers to join the team, it is clear to us that designing systems like ours requires a special skillset. In particular, the ability to work in dramatically different scales and manage relationships between dozens of components.



More Stability
More Stability
Small team. Big difference
It takes a village, but when it comes to ID, I believe small teams work best. For Ion, we had a team of three. Myself as team lead and Robert Hubler and Nick Oakley working as remote contractors in the Pacific Northwest. I’ve worked with both of them for over a decade, so the creative collaboration was easy. In 2017, Rob moved to California and joined Intuitive full time - you can see him standing next to me in the Ion team photo. As you can imagine, inventing and developing a technology like this for use inside the human body is a heavy lift. In the end the Ion team had nearly 500 engineers and clinical experts attending quarterly all-hands meetings.



Sketching
Sketching
the beginning.
“Ramp-up time is about six months” is what GM Chris Carlson told me at the beginning of the project. Thinking back on it, this estimate was conservative. We hit the ground running with a full team of ID, IxD and Visual Design - and pen went to paper immediately…but it took nearly a year of concept development, workshops and labs to even begin to compose the picture of what Ion would become. Nearly a pacific ocean of coffee was consumed.



Introducing Ion 3
Introducing Ion 3
Hands on.
All too often you don’t know what you have until you build it. We alternated between CAD and quick and dirty physical mockups to sort out workflow, features, architecture, ergonomics…everything really. Foam core mixed with higher fidelity 3D print was the tool of choice.



Eyes On
Eyes On
Eyes on.
Working at this scale, VR offered great advantages for design ideation and rapid prototyping. We used it to evaluate Ion in various bronchoscopy suite layouts, to assess range of motion requirements for our monitors, for CMF exploration. What was unexpectedly useful was the ability to change our point of view and experience the product as 5th percentile female (size) or 95th percentile male. This lead to a few revelations.



The Craft
The Craft
evolution.
Constant iteration and the efficient production of physical mockups enabled us to evaluate tradeoffs and push engineering. I often like to describe prototyping like being a time-traveler. We can quickly show the future consequences of certain architecture decisions and use that as a tool for revisiting those choices.



Bring up
Bring up
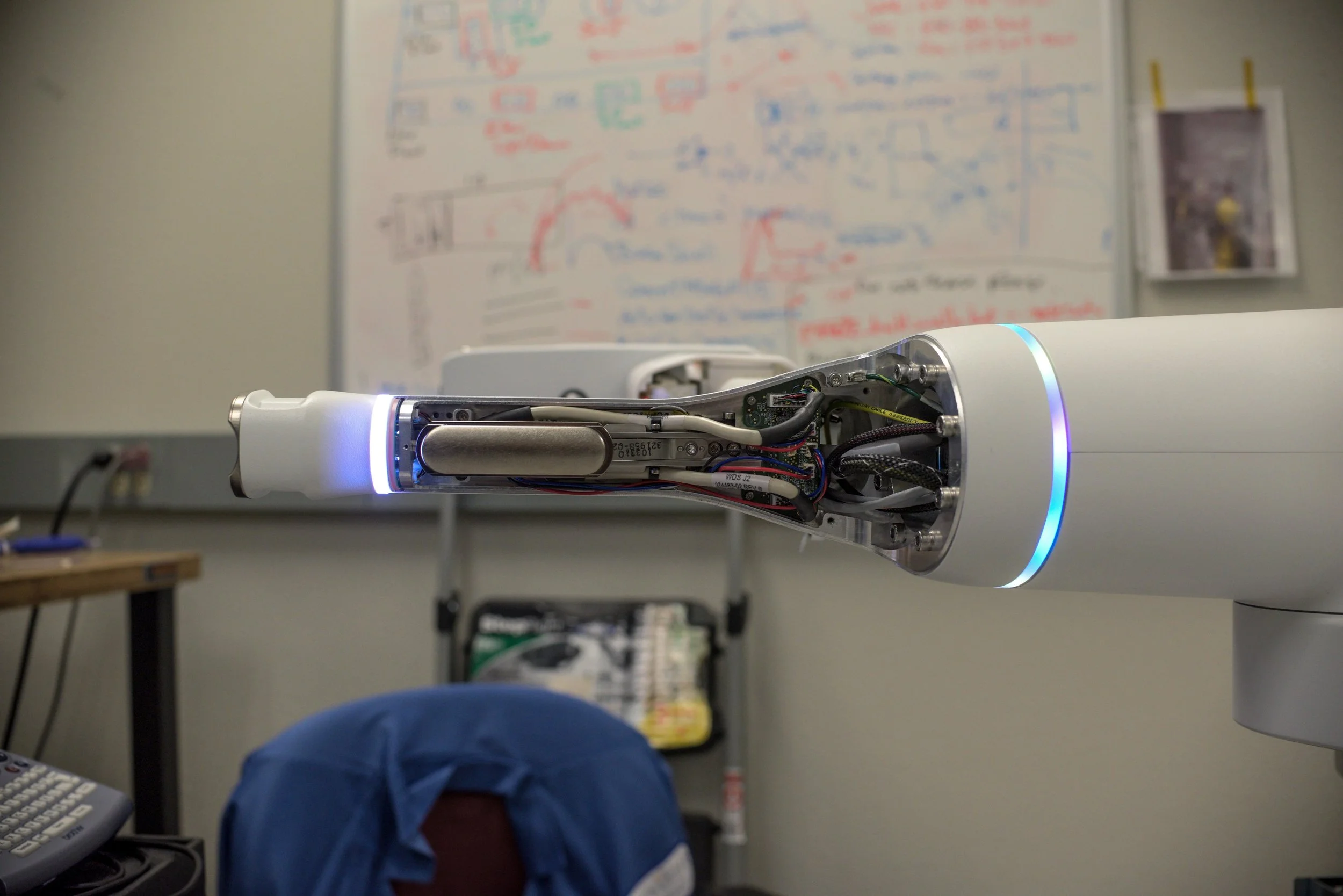
Bring up.
The first Alpha prototypes were assembled and Ion came to life. These prototypes served as a mid-way point for us on the ID team. I believe robotics differs from traditional ID because you can use sensors and motors to alter perceptible physics in unexpected ways. The object becomes dynamic rather than static - and I like to use this dynamism to explore minimalist solutions. We had learned to wait for the functioning system to finish certain things on the design you just can’t get a feel for otherwise.



North Star
North Star
North Star.
We used what we learned from the Alpha to start having a conversation with the engineering team about the details. Rob and I worked over many months with model makers to craft a north star model. This represented our vision for what we might achieve for our first shipping units and all elements were received with a certain brilliant pragmatism and “can do” attitude.



Fabrication
Fabrication
fabrication.
All of the glorious beauty that comes with low volume, high precision manufacturing.



Finish
Finish
finish.
Once we were at the stage where we were rolling systems out to customers, the design work continued as we worked with marketing to tell the story of Ion and advise on how best to feature product attributes.




Ion In Use
Ion In Use
impact.
Since 510k clearance in 2019, Ion has been deployed to hospitals nationwide. The real product is not the Ion system, it’s the impact to patient’s lives that Robotic Navigational Bronchoscopy can enable. Stay tuned as clinical efficacy is documented and published.